Surgery
Recommended for people with curves usually greater than 45º or 50º and/or who are at high risk of continued worsening even after they are finished growing. Curves that grow very large may cause pain, limit certain body functions and cause difficulty or discomfort in breathing. Surgery is almost always a family decision, one that you and your family or guardians will make based on how you feel.
Treatment Goals
- Minimize spinal curvature over the life of the patient.
- Maximize lung function over the life of the patient.
- Minimize the extent of any final spinal fusion.
- Maximize motion of chest and spine.
- Minimize complications, procedures, hospitalizations and burden for the family.
- Consider overall development of the child.
If I need scoliosis surgery, what can I expect?
In adolescent idiopathic scoliosis, the primary surgery used today is fusion surgery. In this surgery, metal implants are attached to the spine and then connected to a single rod or 2 rods. This configuration holds your spine correction in place until the vertebrae fuse together into the corrected position. The incision is usually made in your back, but can be made in the front if you have a single thoracic (middle or middle-upper back) or a single lumbar (lower back) curve. The surgery will take several hours to complete. Patients usually stay in the hospital for 3 to 6 days after the surgery. As new, promising surgical procedures are being studied and tested, spinal fusion remains the prevalent and most enduring procedure to date. Your surgeon will discuss all the specifics of your surgical options with you, and can answer all of your questions.
Will surgery only stop my curve from growing or will it help straighten it?
Spinal fusion surgery should stop your curve from growing and will very likely also significantly improve the curvature.
How long will it take me to recover from surgery?
Everyone recovers differently, but here is what typically occurs:
| 3-6 days post-surgery: | Leave hospital |
| 10-14 days post-surgery: | Discontinue pain medication |
| 3-4 weeks post-surgery: | Return to school |
| 7 days - 6 months post-surgery: | Gradually return to activities |
| 6 months post-surgery: | Resume full participation in all activities |
Surgery Techniques
In Situ Spinal Fusion
This procedure fuses together vertebrae to stop progression of scoliotic curves.
- In situ fusion means that the curve will be fused "where it is" with little or no correction of the spine. The goal is to address the curvature early, before it becomes severe (e.g., a child with a 40°curve that has a poor prognosis).
- It is performed from the back (posteriorly), through the chest (anteriorly), or through a combined approach.
- Sometimes instrumentation (rods, hooks, and screws) may be placed to help straighten the spine slightly and act as an internal brace for the bone graft—which replaces the spine joints—that will form the fusion mass, or one solid piece of bone.
- When instrumentation is not used, usually in young children, the child may need to wear a brace, or be placed in a cast, following the operation. In general, in situ fusion is a safer procedure than those that provide more correction in the curvature of the spine.
Hemi-Epiphysiodesis
Aimed at stopping abnormal growth on one side of the spine with the hope that continued growth on the other side will correct the curve over time.
- Every curve has a concave and convex side. If the growth centers are removed and spinal fusion is performed on the convex side, the concave side might continue to grow, possibly improving the curve.
- In young children, this procedure can be challenging and unpredictable. This procedure is typically done for patients with congenital curves (where the bones are not normally formed).
Hemivertebra Resection
An indication for young children with scoliosis with abnormally shaped vertebrae (triangular vs. rectangular) in their spine who have a “trunk lean” or a progressive curve.
- In a resection, hemivertebra(e) may be removed from the front, back, or both parts of the spine, depending on the child's situation.
- Once a hemivertebra is removed, the vertebrae above and below it are fused together, often with instrumentation.
- Most children will wear a brace or cast after the operation until the spine heals.
- This operation has inherent risks, including bleeding and neurologic injury, but good spinal correction is often achieved.
Spine and Rib-Based Growing-Rod Operation
Uses a spine-based or a rib-based system (i.e., VEPTR) where the curve is spanned by 1 or 2 rods under the skin to avoid damaging the growth tissues of the spine.
Rods are attached to the spine or ribs above and below the curve with hooks or screws at either end of the rod. Limited fusion is performed at each of the hook/screw foundation sites.
- The curve can usually be corrected by 50% at the time of the first operation.
- After the rods are implanted, patients are prescribed a special brace to wear for several months.
- The child then returns every 6 months to have the rods "lengthened" until the spine is closer to maturity. This procedure is typically performed on an outpatient basis with the implants being made through a small incision. These frequent surgeries, mostly through the same incision site, can cause infection in the skin tissue susceptible and other skin problems.
- When the child becomes older and the spine has grown, the doctor will remove the instrumentation and perform a formal spinal fusion operation.
- In the past, this procedure had a very high complication rate, most of which were related to the instrumentation (hook dislodgment, rod breakage/fractures). Newer techniques are more promising as treatment with growing rods remains a long therapy for the child.
- Doesn't interfere with normal spinal growth and may even have a potential for growth stimulation beyond the expected growth rate.

Figure. Growing rods are a spine-based system where the curve is spanned by one or two rods under the skin to avoid damaging the growth tissues of the spine. The rods are attached to the spine above and below the curve with hooks or screws at either end of the rod.
Magnetically Controlled Growing Rod (MCGR) Procedure
The idea of non-invasive multiple lengthening without the need for anesthesia and open surgery is appealing given the direct relationship between high complications and repeated surgeries.
- These devises allow for lengthening to be performed in the doctor's office.
- They are composed of an implantable rod, an external remote controller (ERC) and accessories. The titanium rod includes a telescopic actuator portion that holds a small internal magnet. Rotation of the magnet remotely by use of the ERC causes the rod to be lengthened or shortened. The rod is implanted and secured using standard fixation components, such as hooks and/or pedicle screws as anchors.
- Magnet driven rods are now being used for select patients and preliminary results have shown to be able to reduce morbidities, cost, and decrease stress for patients and parents.
- They have been implanted in cases of both idiopathic and neuromuscular scoliosis.
- Unlike distraction techniques (growing rods), repeated surgeries are not required.
- The Luque trolley uses wires to allow the spine to grow in the desired direction as the wires slide along contoured rods.
- In the Shilla technique initial correction is achieved by instrumentation and fusion at the apex, or most deformed portion of the spine. Specially designed screws are placed at the ends of the curve and slide along the contoured rods guiding the direction of the spine as it grows. Patients who have undergone the Shilla technique are usually placed in a special brace for 3 months after the surgery.
Compression-Based Growth-Friendly Surgery
Intended to produce relative growth inhibition on the convex side of the curve.
- This technique can be used in children who are still growing, have a progressive curvature that measures less than 35º, and who are able to tolerate open or endoscopic exposure of the spine.
- By placing special vertebral body staples or tethers on the convex side of the curve, growth is inhibited on that side. The idea is that the scoliosis may then correct through more growth on the concave side of the curve.
Anterior Spinal Fusion with Instrumentation
May be performed in addition to the posterior approach, depending on the surgeon's determination of how much growth may remain for the patient.
- Performed through an incision in the patient's side or rib cage, or through small incisions between the ribs, aided by a camera (thoracoscopic fusion).
- Mitigates the "crankshaft phenomenon”, which is curve progression that can occur after posterior (rear) fusion due to continued growth of the vertebrae. (Curves sometimes continue to grow by rotating around the original surgical fusion.)
- Typically performed around the same time (shortly before or after) as the definitive posterior operation.
- The decision to undergo the additional (anterior) surgery required to prevent crankshaft curve progression is dependent on the age of the child at the time surgery is selected.
Posterior Spinal Fusion with Instrumentation
Performed to stop curvature of the spine and achieve permanent correction. The procedure provides permanent stabilization in the corrected position by removing the joints between the vertebrae to be fused.
- All the vertebrae involved in the curve are prepared and bone graft (either from the pelvis, ribs, or from the bone bank) is placed in each space resulting from joint removal.
- Over time (4 to 6 months), the graft adheres to the vertebral bone, and the operated portion of the spine heals into a solid block of bone which cannot bend, thus eliminating further progression of the curve.
- Typically, in a child who has reached an appropriate age for definitive fusion, instrumentation will also be placed when the fusion is performed. The instrumentation rigidly “fixes” the spine internally through rods being attached to screws, hooks and wires (“anchors”) at multiple sites along the curve so that the corrected position is carefully preserved while the fusion is completed over a 4- to 6-month period.
- Depending on the flexibility of the curve and any preceding treatment (such as traction), there may even be additional correction of the curve achieved by the application of the instrumentation.
- Often the patient does not need a cast or brace if the internal instrumentation is felt to be adequate at the time of surgery.
Conditions for Surgery
Early Onset Scoliosis
Surgery is generally recommended if brace or cast treatment should fail to keep the scoliosis from progressing, or if the curve pattern does not appear amenable to brace or cast treatment.
The dilemma faced by the surgeon is how to stop the progression of a curve without adversely affecting future growth. Various growth-friendly surgeries are designed to follow the principles of EOS treatment outlined earlier, allowing the spine and lungs to grow while controlling spine and lung problems. Generally, this type of surgery may be divided classified as Distraction-Based, Guided Growth, and Compression Based.
Adolescent Idiopathic Scoliosis
Adolescent Idiopathic Scoliosis
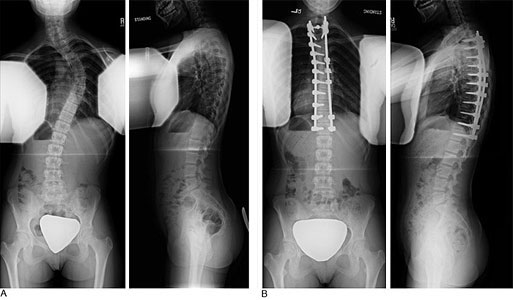
Figure 7. A) Front and side x-rays of a patient with adolescent idiopathic scoliosis in her thoracic spine. B) Postoperative correction through a posterior approach using 2 rods and pedicle screws.
Surgical treatment is often recommended for patients whose curves are greater than 45° while still growing, or are continuing to progress greater than 45° when growth stopped. Fusion surgical treatment today uses metal implants that are attached to the spine, and then connected to a single rod or two rods. Implants are used to correct the spine and hold the spine in the corrected posi-tion until the instrumented segments fuse as a bone. The goal of surgery is to:
- Prevent curve progression
- Obtain some curve correction
The surgery can be performed with either a posterior or anterior approach:
- Posterior approach: A straight incision is made along the midline of the back (See Figure 7). This approach is used most often in the treatment of AIS and can be effective for all curve types.
- Anterior approach: A similar (straight) incision is made through front of the spine (anterior ap-proach (Figure 8). This approach is an option in cases where a single thoracic curve or a single lumbar curve is being treated.
Post-surgery typical timeline:
- 3-6 days: Hospital stay
- 10-14 days: Most children will no longer need pain medications
- 3-4 weeks: Patient can perform regular daily activities and typically returns to school
- 3-6 months: Depending on the patient’s activities, full participation is allowed.

Figure 8. A) Front and side s-rays of a patient with adolescent idiopathic scoliosis in her thoracic and lumbar spine. B) Post-operative x-rays showing instrumentation placed via an anterior (side) approach.
Juvenile Idiopathic Scoliosis
Vertebral body stapling and tethering are novel options for treatment at this time.
Neuromuscular Scoliosis
The type of spinal stabilization depends on the age of the patient, ambulatory status, and underlying condition. Surgical goals are:
- Prevent curve progression
- Improve sitting balance and tolerance (in non-ambulators)
- Reduce repositioning
- Reduce pain
Thoracic Insufficiency Syndrome (TIS)
Thoracic Insufficiency Syndrome (TIS)
A new surgical technique—VEPTR (vertical expandable prosthetic titanium rib) thoracoplasty—treats the combined thoracic abnormality (spine/rib cage) in skeletally immature patients by enlarging the constricted chest and straightening the spine indirectly without a spine fusion. VEPTR surgery is extensive. Devices are placed under the scapula (shoulder blade) and are attached to the ribs near the neck and continue down to either the spine, or the ribs near the waist to help stabilize the surgically expanded chest wall constriction (expansion thoracoplasty).
To accommodate later growth, the devices are expanded twice a year in outpatient surgery through small incisions. Some centers are using the VEPTR device as a means to straighten the spine indirectly via the ribs and chest wall. Long-term follow-up studies of this technique are underway. Currently, there are a limited number of institutions offering VEPTR surgery. Your child's spine surgeon can advise whether your child's condition is appropriate for VEPTR treatment and provide referral information, if needed.
Developmental Kyphosis
Spinal Fusion
If kyphosis has become severe (greater than 80°) and causes frequent back pain, surgical treatment may be recommended. Surgery provides significant correction without the need for postoperative bracing. Pedicle screws, hooks, or sublaminar cables are placed, two per level, and connected with two rods.
Most surgeries are performed from the back; however, some physicians may recommend additional surgery on the front of the spine. Patients are usually able to return to normal daily activities within four to six months following surgery. (Figure 4).
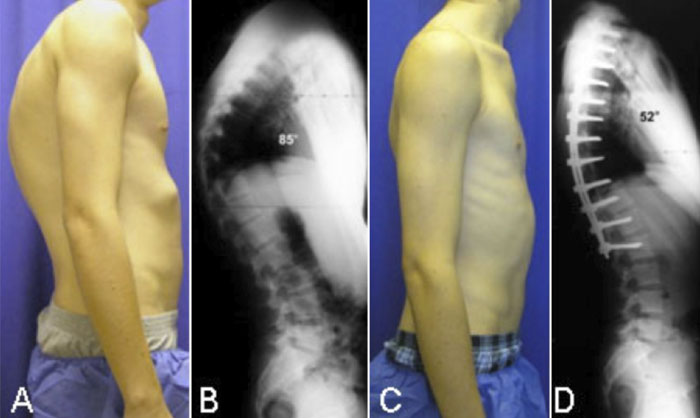
Figure 4. A) Preoperative photo of patient with severe kyphosis secondary to Scheuermann's disease. B) Preoperative x-ray of the same patient. C) Postoperative photos of the same patient one year after surgical correction of the kyphosis. D) Postoperative x-ray of the same patient.
Moderately flexible curves often straighten simply from lying face down during surgery; however, rigid curves may require additional surgical intervention, such as Smith-Peterson osteotomies.
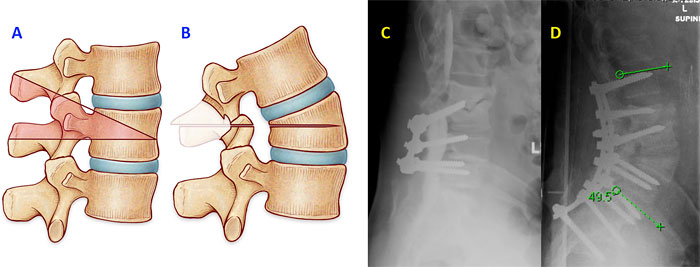
Smith-Peterson Osteotomy
The Smith-Peterson osteotomy involves cutting the bone to improve vertebral alignment; as a result, every spinal segment included in the osteotomy is limited in extension (backward bend) by two sliding facet joints. If these joints are removed and the disc in front is mobile, it is possible to achieve 5° to 10° additional extension, per level. (Figure 5).
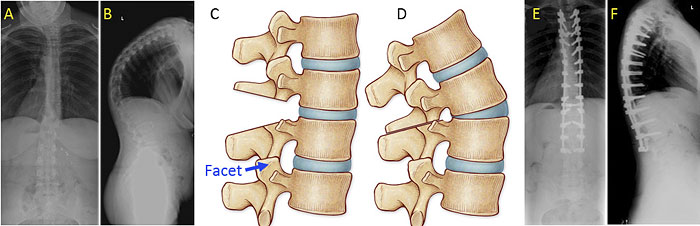
Figure 5. A) & B) Front and side x-rays of a person with severe, rigid Scheuermann's kyphosis. C) Illustration of a side view of the spine showing how the facet joints are removed. D) After the facets are removed, the spine can be tilted backward. E) & F) Front and side x-rays after surgery.
Post-Traumatic Kyphosis
For traumatic kyphosis that is significant, surgery may the best option for safeguarding quality of life in the future.
- Posteriorspinal fusion with instrumentation is the primary surgical treatment for traumatic kyphosis. The surgeon enters the operative area through the back.
- Anterior-posterior spinal fusion entails 2 incisions, 1 in the front of the body and another in the back.
- Osteotomy, on occasion, may also be necessary to restore alignment. The procedure entails cutting through bone (and possibly removing bone as well).
Spondylolysis
If the pain, spasm, or slippage increases despite conservative management, then the surgeon may discuss several potential surgical options with the patient:
1) Spinal fusion (for spondylolisthesis)
- For a majority of children and adults, fusing the fifth lumbar vertebra to the sacrum (the most common vertebrae involved in adolescents with spondylolisthesis) is the preferred surgical option.
- The fusion involves removing the loose bony fragments and placing bone graft that will lead to the 2 vertebrae “fusing together" to prevent any further slippage. Specially designed screws and rods may be needed to hold the vertebrae in place to help the two bones fuse together.
- A perforated, hollow cylinder called a “cage” is sometimes required. The “cage” is filled with bone matter and placed in the disc space between the two vertebrae to increase the likelihood of fusion.
- Bones may be realigned depending on how much one vertebra has slipped forward on the other. The most important steps are restoring stability and making sure the nerves have no pressure on them.
2) Pars repair
At times the pars fracture can be repaired without fusing 2 vertebrae together. This involves removing any scar material that may have developed in thefracture site of a single vertebra, and stabilizing the 2 sides of the fracture to restore normal anatomy.
Bones are not fused together. The rigid or problematic bone is removed; 2 sides of the fracture are stabilized to restore normal anatomy.
- Rarely successful in adults 20 years and older
- Not recommended if there is slippage (spondylolisthesis) or moderate or severe disc degeneration at that vertebra level.
Spondylolisthesis
If the pain, spasm, or slippage increases despite conservative management, then the surgeon may discuss spinal fusion with the patient:
- For a majority of children and adults, fusing the fifth lumbar vertebra to the sacrum (the most common vertebrae involved in adolescents with spondylolisthesis) is the preferred surgical option.
- The fusion involves removing the loose bony fragments and placing bone graft that will lead to the 2 vertebrae “fusing together" to prevent any further slippage. Specially designed screws and rods may be needed to hold the vertebrae in place to help the two bones fuse together.
- A perforated, hollow cylinder called a "cage" is sometimes required. The "cage" is filled with bone matter and placed in the disc space between the two vertebrae to increase the likelihood of fusion.
Bones may be realigned depending on how much one vertebra has slipped forward on the other. The most important steps are restoring stability and making sure the nerves have no pressure on them
Adult Idiopathic Scoliosis
Surgical treatment is reserved for patients who have:
- Failed all reasonable conservative (non-operative) measures.
- Disabling back and/or leg pain and spinal imbalance.
- Severely restricted functional activities and substantially reduced overall quality of life.
The goals of surgery are to restore spinal balance and reduce pain and discomfort by relieving nerve pressure (decompression) and maintaining corrected alignment by fusing and stabilizing the spinal segments. When patients are carefully chosen and mentally well-prepared for surgery, excellent functional outcomes can be achieved which can provide positive life-changing experience for a given individual patient. When larger surgeries—those greater than 8 hours—are necessary, surgery may be divided into 2 surgeries 5 to 7 days apart. Surgical procedures include:
- Microdecompression relieves pressure on the nerves; A small incision is made and magnification loupes or a microscopic assists the surgeon in guiding tools to the operation site. This type of procedure is typically used only at one vertebra level, and carries a risk of causing the curve to worsen, especially in larger curves >30 degrees.
- Surgical stabilization involves anchoring hooks, wires or screws to the spinal segments and using metal rods to link the anchors together. They stabilize the spine and allow the spine to fuse in the corrected position.
- Fusion uses the patient's own bone or using cadaver or synthetic bone substitutes to "fix" the spine into a straighter position
- Osteotomy is a procedure in which spinal segments are cut and realigned
- Vertebral column resection removes entire vertebral sections prior to realigning the spine and is used when an osteotomy and other operative measures cannot correct the scoliosis.
Adult Degenerative Scoliosis
Surgical treatment is reserved for patients who have:
- Failed all reasonable conservative (non-operative) measures.
- Disabling back and/or leg pain and spinal imbalance.
- Severely restricted functional activities and substantially reduced overall quality of life.
The goals of surgery are to restore spinal balance and reduce pain and discomfort by relieving nerve pressure (decompression) and maintaining corrected alignment by fusing and stabilizing the spinal segments. When patients are carefully chosen and mentally well-prepared for surgery, excellent functional outcomes can be achieved which can provide positive life-changing experience for a given individual patient. When larger surgeries—those greater than 8 hours—are necessary, surgery may be divided into 2 surgeries 5 to 7 days apart. Surgical procedures include:
- Decompression surgery removes the roof of the spinal canal (laminectomy) and enlarging the spaces where the nerve roots exit the canal (foraminotomy), resulting in decompressed nerve roots and pain relief. Typically only used at one or two vertebral levels in patients with leg pain from stenosis and smaller curves (< 30 degrees). In patients with more than two levels of stenosis and larger curves >30 degrees, a decompression without fusion has a risk of destabilizing the spine and causing the curve to worsen.
- Surgical stabilization involves anchoring hooks, wires or screws to the spinal segments and using metal rods to link the anchors together. They stabilize the spine and allow the spine to fuse in the corrected position, and is always performed with the addition of a fusion.
- Fusion uses the patient's own bone or using cadaver or synthetic bone substitutes to "fix" the spine into a straighter position
- Osteotomy is a procedure in which spinal segments are cut and realigned
- Vertebral column resection removes entire vertebral sections prior to realigning the spine and is used when an osteotomy and other operative measures cannot correct the scoliosis
Age-Associated Hyperkyphosis
If these conservative measures do not help, surgery may be necessary to control pain and improve curvature or decompress nerve roots.
Scheurmann's Kyphosis
Spinal Fusion
If kyphosis has become severe (greater than 80 - 90°) and causes frequent back pain, surgical treatment may be recommended. Surgery provides significant correction without the need for postoperative bracing. Pedicle screws are placed, 2 per vertebra, and connected with 2 rods. This process promotes gentle straightening of the spine. Most surgeries are performed from the back; however, some physicians recommend additional surgery on the front of the spine. Patients are usually able to return to normal daily activities within 4 to 6 months following surgery.
Smith-Peterson Osteotomy
Moderately flexible curves often straighten simply from lying face down; however, rigid curves may require surgical intervention. The Smith-Peterson osteotomy involves cutting the bone in the back of the spine that connect the facet joints. The removal of this bone and the joints allows the spine to move backwards into extension or more of an upright position. This type of osteotomy is commonly performed during the surgical treatment of Schuermann's kyphosis.
Adult / Fixed Sagittal Imbalance (flat-back syndrome)
Adult / Fixed Sagittal Imbalance (flat-back syndrome)
The decision process for surgery depends on: the type of sagittal imbalance, a history of prior surgeries, the degree and location of neural compression, the age and health of the patient, and more.
Posterior osteotomy (also called "Smith-Peterson" or "Ponte" osteotomy)
This procedure involves removing facet joints and certain ligaments. The facet joints typically limit extension of the spine so their removal (posteriorly) allows the surgeon to accentuate lordosis by tilting the bones through a mobile disc space. Over multiple levels, 5o to 15o of lordosis per level is possible.
Posterior Osteotomy:
A) A side view of the spine showing the bone and facet resection.
B) A side view after the osteotomy is closed.
C) A lateral (side) radiograph of a woman with severe, rigid, Scheurmann's kyphosis.
D) A lateral x-ray after surgery. Multi-level posterior osteotomies allowed the surgeon to reduce the kyphosis to normal levels.
Pedicle subtraction osteotomy
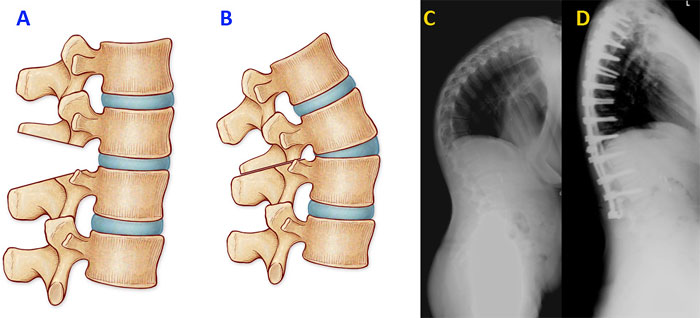
Surgeons use this procedure to cut through segments of the spine causing sagittal imbalance. Known as a "closing wedge osteotomy", a triangle of bone is removed so the bone can be angled backwards. (The technique similar to placing a wedge between bricks, creating a sudden backward bend in the spine.) The procedure is particularly powerful, especially in the lumbar spine where the bones are bigger, and small corrections can lead to large improvements in posture. The surgery requires the support of instrumentation above and below the osteotomy and is a major surgery with relatively high rates of complications.
Pedicle subtraction osteotomy:
A) A side view showing the area of bone resection in pink.
B) The lordotic segment after the osteotomy is closed. Note how the front of the vertebra is twice the height of the back causing lordosis.
C) The preoperative x-rays of a patient with fixed sagittal imbalance due to bone settling and infection.
D) A lateral (side) x-xrayray showing the restored lordosis after the osteotomy.
Vertebral column resection
The most powerful (and invasive) of all spinal osteotomies, the vertebral column resection is necessary when there is a sharp, severe bend in a small area. It involves essentially dislocating the spine in a controlled manner and realigning it in the proper direction.
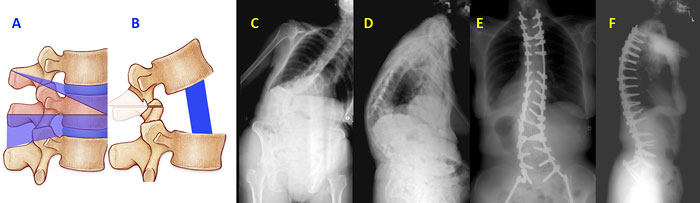
Vertebral column resection:
A) A side view of the spine showing the additional bone removed beyond a pedicle subtraction osteotomy (added area in blue).
B) A strut graft or cage is placed between the cut vertebra.
C) & D) The front and side view of a woman with severe, rigid kyphoscoliosis.
E) & F) Postoperative front and side x-rays after the realignment procedure.
Anterior-posterior osteotomy
Like the vertebral column resection the anterior-posterior also, in essence, the anterior-posterior osteotomy (APO) dislocates the spine so that it can be repositioned properly. In an APO, he back section of the bone is removed from the back of the spine, and the front portion is removed from a separate anterior incision. The anterior-posterior osteotomy has the same effect as a vertebral column resection, but it avoids risky surgical navigating around the nerves to remove the vertebra.
Osteoporosis & Compression Fractures
Osteoporosis & Compression Fractures
May be necessary to control pain, in rare instances, to stabilize the structure of the spine, or decompress the nerve roots or spinal cord. New techniques to treat the problem of compressed vertebrae include:
- Vertebroplasty involves an injection of bone cement into vertebrae to improve the strength of the bone.
- Kyphoplasty, similar to vertebroplasty, except that a balloon is inflated in the vertebra to create a space before the filling with bone cement. Both procedures require at least sedation and local anesthesia but sometimes require general anesthesia. With both procedures, very tiny incisions are made under x-ray control. As with any other surgical procedure, there are certain risks.
Degenerative Discs & Facet Joints
Degenerative Discs & Facet Joints
May be required to alleviate pain associated with severe and progressive degenerative changes. Potential surgeries are:
- Spinal Fusion (the connection of two vertebra) with (hooks, rods, and/or screws) or without, and the use of bone grafts or bone graft substitutes to allow the two vertebra to weld together. The complete healing of a fusion can take 3-6 months and heals in a similar way as a broken bone.
- Posterior Lumbar Laminectomy/Decompression removes part of the vertebral layer and facet joints to reduce pressure on the nerves in the spine and the associated pain.
Spinal Stenosis
Surgical decompression of the involved vertebrae allows patients to walk farther and stand longer without pain.
- Decompression surgery removes the roof of the spinal canal (laminectomy) and enlarging the spaces where the nerve roots exit the canal (foraminotomy). The result is decompressed nerve roots and pain relief.
- Vertebral fusion may be necessary (often in conjunction with decompression surgery) if instability is present. The spinal fusion joins together and heal spinal segments fusing bone, either from the pelvis (iliac crest) or from the bone bank (donated bone). In the majority of cases, a metal implant consisting of screws and rods is used to help maintain stability at these segments while the fusion heals.
The hospital stay is generally shorter if spinal fusion is not performed and a bit longer if it is. In either case, particularly if a patient’s condition had debilitated rapidly preoperatively, a short stay in a rehab facility to regain strength and mobility may be needed. The actual details of post-discharge care, resumption of normal physical and athletic activities, driving, and the possible use of a brace will be provided by the patient's surgeon.
Herniated or Ruptured Lumbar Disc
Herniated or Ruptured Lumbar Disc
If 6 weeks to 3 months with non operative measures does not produce symptom improvement, or if leg pain or weakness persists or worsens, surgical treatment may be suggested. The most common procedure for this condition is a discectomy in which a small incision is made in the back and the herniated portion of the disc is removed. Relief of symptoms is often quite dramatic. Healthy patients can have this surgery in an outpatient setting, but occasionally the side effects of anesthesia and pain medication used postoperatively require admission to the hospital for a 1 to 2 days. After the surgery, some recovery is necessary, but gradual return to full activities is the rule. The time it takes to return to work and sports activities varies and should be discussed with the patient's surgeon.
Cervical Degenerative Disc Disease
Cervical Degenerative Disc Disease
If the symptoms are significant and persistent after nonoperative measures and/or a significant neurological deficit is apparent, surgical treatment is often necessary.
- Anterior cervical discectomy and fusion is most commonly performed for cervical degenerative disc disease and can also include removal of the degenerative bony spurs that occur around the border of the discs. The fusion is performed with either bone from the pelvis (iliac crest) or from the bone bank (donated bone), and the vertebrae are usually fixed together using a metal plate and screws.
- Posterior decompression and stabilization might be performed as an alternative to anterior cervical discectomy, if multiple levels are involved. This procedure uses plates and screws, and may also require a fusion.
Conditions That Share Treatment Type With EOS
Patient Videos
Find A Specialist
Although SRS does not recommend or refer physicians, members that may be available for a consultation are listed on the physician locator.
Patient Stories
Explore the stories to learn more about patients with various spinal disorders.